The state of health science in the US today is not weak, but it is under threat. The main problems: 1. p-value hacking. 2. commoditization of adjunct and postdoc labor. 3. disincentives of null value results or replication. All of these things threaten the foundations of the increasingly unsustaiunable edifice that is modern health science, and all of them derive in one way or another from the same root problem: the only source of objective funding, untainted by corporate interests, is the NIH. In essence, health science is a zero-sum game.
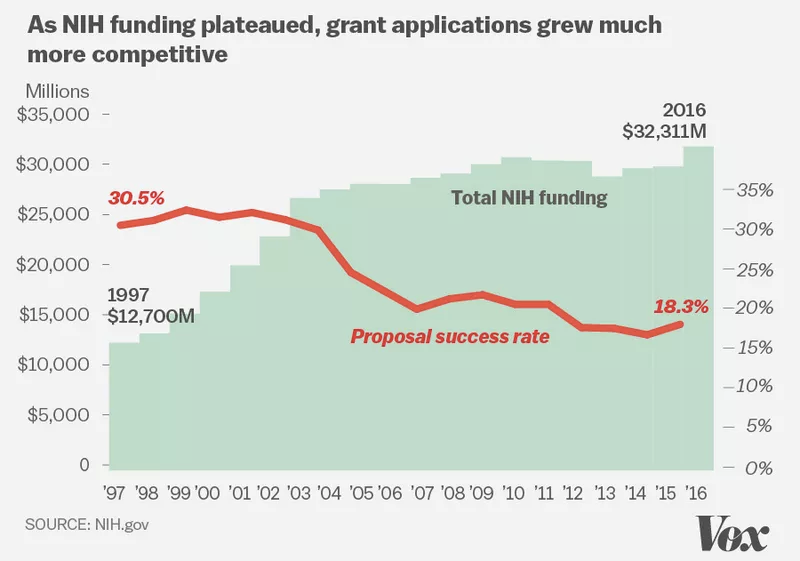
This is why the Trump Administration preliminary budget proposal is ominous: it specifies an unprecedented 18% cut to the NIH budget.
As the image above illustrates, grant applications have grown almost twice as competitive over the years as NIH funding stayed constant. An 18% cut in this context is like an amputation.
There is only one possible outcome of this: labs will shrink. Health science research is going to be dramatically curtailed. Maybe there are benefits, in the long run, to this – but in the short run it will only worsen – severely – the problems that health science research currently faces. The question is, how resilient is the health science establishment? We are going to find out.
Related: great article at The Atlantic that points out how private funding is a drop in the bucket compared to government support. In my opinion, public science funding is as critical and as irreplaceable as national defense.
I try to stay out of political theory on this blog, but Vox Day’s essay on the differences between the “VHIQ” and the “UHIQ” struck me as intellectually interesting enough that I felt like exploring it further. Personally, I don’t know what my IQ is, so that means I am merely above average*, since only people with very/ultra-high IQ seem to be motivated to willingly take the test. VD lists a number of plausible qualitative traits, of which the following caught my eye:
VHIQ inclines towards binary either/or thinking and taking sides. UHIQ inclines towards probabilistic thinking and balancing between contradictory possibilities.
…
VHIQ is uncomfortable with chaos and seeks to impose order on it, even if none exists. UHIQ is comfortable with chaos and seeks to recognize patterns in it.
…
VHIQ is competitive. UHIQ doesn’t keep score.
VD later goes on to quote Wechsler, the founder of the IQ test, at length and summarizes:
Wechsler is saying quite plainly that those with IQs above 150 are different in kind from those below that level. He is saying that they are a different kind of mind, a different kind of human being.
The division into binary groups here – “normal human” (sub-150 IQ) and the Next (150+), and then at the next iteration between VHIQ and UHIQ, is confusing to me, particularly since it is IQ itself being used to classify people into the binary choices. In the comments, VD clarifies (?) that “It’s entirely possible for a 175 IQ to be VHIQ and for a 145 IQ to be UHIQ” but that just moves the binary classifying to a relative scale than an absolute one. Since he also asserts that you need to be at least +3 SD (ie, IQ of 145) to even qualify as VHIQ, it’s clear that the numbers do matter.
There’s a glaring circularity here that I am doing a poor job of articulating. I’ll just make note of it and move on.
VD’s excerpted passage from Wechsler is, however, nonsense. He created an empirical test, intended to assess “varying amounts of the same basic stuff (e.g., mental energy)” and then made it into a score. I have worked with neurologists before and they make the same category error that psychologists like Wechsler do, in ascribing quantitative rigor to tests like the Expanded Disability Status Scale (EDSS). Just because you can ask someone a bunch of qualitative questions and then give them a “score” based on a comparison of their answers to those of a “baseline” person, does not mean you have actually magically created a quantitative test. Wechsler’s very use of the word “quantitative” is an abuse of language, a classic soft-sciences infatuation with concepts best left to hardsci folks. There’s nothing quantitative about the WAIS whatsoever, until you look at aggregate results over populations. Wechsler lacked even a basic understanding of what human cognition’s base units might be – certainly not hand-wavy bullshit like “mental energy”. Volumetric imaging with DT-MRI is probably the only actual quantitative method the human race has yet invented to probe that “basic stuff” of which Wechsler dreams; but there are some serious engineering constraints on how far we can go in that direction.**
Human cognition isn’t so easily captured by a single metric, even one built on such muddy foundation as the WAIS. It’s chaotic, and emergent, and inconsistent. This infatuation with pseudo-qualitative testing isn’t limited to WAIS; people overuse Meyers-Briggs and over-interpret fMRI all the time. Do qualitative metrics like WAIS or EDSS have value in certain contexts? Of course. However, as a signpost towards Homo Superior, it’s no better than Body Mass Index.
* Why bother with false modesty? I do have a PhD in an applied physics field, after all, and I scored higher than VD on that one vocab test, so empirically it seems reasonable to suppose I am somewhat ahead of the curve.
** spouting off about fMRI in this context is a useful marker of a neurosci dilettante.
A change in US labour regulations will render many postdocs eligible for overtime pay — and create an incentive to raise their wages. The law may ultimately mean fewer postdocs. But some say that the policy could spark much-needed changes to a research system that relies heavily on postdocs yet offers them few opportunities for career advancement.
The new rule, finalized on 18 May by the US Department of Labor, will make overtime pay mandatory for many postdoctoral researchers who make less than US$47,476 per year. Overtime, which is paid at 1.5 times the normal hourly wage, kicks in once workers exceed 40 hours on the job in one week.
The problem, as the article itself points out, is that it’s relatively painless for a PI to raise their postdoc salary just enough to meet the minimum required to avoid triggering the overtime requirement. This would mean a raise, but only a few percent, and does nothing to address the broader structural problem facing lack of advancement opportunities for postdocs within the field.
Even if postdocs salaries were raised to 50k across the board – which would have a wonderful impact on distributing postdocs across the country and strengthening science at research institutions nationwide – it would do nothing to alleviate the oversupply of postdocs that is destroying career advancement. Congress can’t really achieve more than incrementalist change like this overtime proposal, but the NIH has far more leverage.
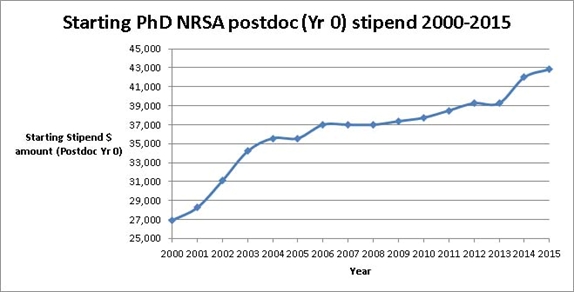
Let’s focus the discussion on fields of bioscience that primarily derive funding from the NIH. The NIH sets its own scale for postdoc pay (fiscal year 2015), for postdoc positions it funds as part of the NRSA fellowship (inherently limited by federal funding for the NIH). These NRSA payscales are then used as a benchmark for universities across the nation to set salary levels for their own postdocs. That level has risen dramatically in the past 15 years, but still falls well short of the NIH’s own pledge of $45k:
NRSA stipends for Year 0 postdocs over time (compiled by the National Postdoc Association)
The NIH imposes salary caps on the amount any given indiovidual may be paid out of an awarded grant. There is no reason the NIH can’t set a minimum level, however – and doing so would not require legislation in Congress and the political process. It would simply be an overnight change.
Imagine for example if the NIH immediately mandated that all postdoc salaries funded by R1 grants had to be funded at 150% of the current NRSA level. Likewise, graduate student support could be immediately mandated as 100% tuition plus stipend. The actual amount of funding however would not change – just the allocation of how that (taxpayer) money is spent. (This would have to apply to all new grants effective the next fiscal year, and not affect currently-funded grants).
The immediate effect would be that fewer graduate students and postdocs could be supported. This would have many downstream ripple effects, but the biggest one would be an exodus of highly trained individuals from academia into other fields and industry, and entrepreneurship. This sounds like a bad thing for science, but the bottom line is that science has progressed on exploited labor for far too long. There are other areas of reform that need to follow, including paying institutional overhead out of grants and the adjunct faculty problem. But those are going to require a. substantial legislative solutions for which there isn’t the political will (because it will cost taxpayer money), and b. self-organization towards unions and collective bargaining, for which there isn’t professional will (because it will require the threat of strikes). Bluntly, science achieves what it does by treating its most valuable assets as commodities. It’s time to revalue, and that will require significant effort. The issue of underpaid postdocs and PhD students is one that is relatively easy to solve, and in doing so will provide much-needed impetus towards those other problems.
I think that solving those issues will in turn lead to solving the other great problem science faces, namely the output problem. But that’s a topic for another day.
(meta: I’ve retired my old science blog, Reference Scan, and have imported the content here. Feel free to browse the Reference Scan category for older posts!)
The 2nd annual accelerated imaging workshop at UW Madison is next week, and should be a great event. There are scheduled speakers from Mayo Clinic, Northwestern, UIUC, Berkeley, Harvard, the NIH, and GE Healthcare (among others). If you think you might be able to attend, the free registration deadline is Saturday June 12th, otherwise you can register on-site for a nominal fee. Here’s the registration form, which you can fax or email in.
Objectives of this workshop are to discuss the current state of the art accelerated imaging concepts and applications, roadblocks to clinical applications and strategies to effectively address these limitations.
Fundamentals of the Constrained Reconstruction Rainbow
State-of-the-Art Concepts and Applications in MRI and other modalities
Rapid Quantitative Imaging
Performance Metrics – Connecting Imaging Science with Radiology
New Hardware Developments
Invited speakers will present keynote lectures on pertinent topics with further presentations by contributed papers. The workshop in Madison will also be tailored towards students’ education.
Extended poster viewing and discussion sessions are an integral part of the scientific program and will allow discussions about new concepts.
The workshop will take place in Madison, WI at the Health Science Learning Center (HSLC), which is located on the University of Wisconsin-Madison campus adjacent to the UW Hospital & Clinics.
The workshop announcement in pdf format can be found here.
If you don’t want to download the PDF of the program, I’ve embedded it below the fold. Also check out the official workshop website on the UW Madison website for more details.
If you attended the ISMRM meeting and were chased out of the poster session by angry Swedes for trying to take photos of the posters, then know that I’ll be uploading my own shots to Flickr later on. However, ISMRM is asking that everyone send their final PPT/PDF files of their posters as printed to posters10@ismrm.org, so they can post those online as well. Hopefully they will ask for these ahead of the meeting, and encourage people during the meeting to do so, next year. I suspect compliance will still be pretty low unless they market this more. Of course, they already have the e-posters, this is just regarding the traditional posters.
Finally, they expect to have video of the oral sessions uploaded to the official site (http://www.ismrm.org/10) within a month. So be patient! An incredible resource, well worth waiting for.
Before the ink was dry on the government’s 2007 budget (or even completed for that matter), the Bush administration’s proposal for the 2008 budget was submitted on February 5th, and the news for biomedical researchers was not very good. According to sources the NIH is slated to receive a $500 million budget cut, before inflation is factored in—assuming a bill inflating their budget for 2007 passes through congress.
Making this even more dire for biomed researchers is the fact that over 10,000 NIH extramural grants are up for renewal in 2008. Those contending for extensions or renewals of such grants are now faced with double difficulty: less money to go around and more people vying for the same number of spaces. Constraints such as these have driven the average age of first-time grant recipients to over 40 years old, barely a young researcher anymore.
The simple truth is that the NIH is probably the single greatest investment of public funds apart from NASA in terms of knowledge generation for the benefit of society that the world has ever seen. Less funds mean less research; less Ph.D.s choosing an academic career; less innovation and less risk-taking. That means more orthodoxy, entrenched and defensive peer-review, and ultimately more echo-chambering.
Even with new funding programs aimed at transitioning postdocs to faculty, it’s hard to justify doing a post-doc to people in the field nowadays – if they have the flexibility, they can make more than double the salary working for industry. What does the future of our field, medical physics and MRI in particular, look like?
The Scientist has released the results of its annual poll and the verdict: MD Anderson Cancer Center in Houston ranks highest, followed by the J. David Gladstone Institutes in San Francisco and the Environmental Protection Agency in the Research Triangle Park. Via Ars,
The most important criteria identified in the survey were access to training and experience that will prove useful, followed by access to books and journals, decent medical insurance, equipment, and the quality of the principal investigator. I’m not sure you’d find many postdocs who would disagree with these; if you’re going to spend three years of your life working on a project, then one would hope the skills and techniques learned would stand you in good stead in the future. Access to the scientific literature is vital, and if you’re not getting paid the earth, the ability to see a good doctor if you get sick is nice.
Least important on the list of concerns was the opportunity to advance within the department, followed by administration issues. Again, this is probably due to the way academic careers work, where it’s beneficial to move from one institution to another for different stages of your career, that way maximizing exposure to the broadest range of techniques, methods and approaches to science. Some institutions are also notoriously reticent about promoting their own postdocs into faculty positions.
Did anyone else see this article? I came across it on msnbc.com – “Scientists Try to Predict Intentions: using brain scans to read minds before thoughts turn into actions” (http://www.msnbc.msn.com/id/17464320/)
I haven’t read anything Dr. Haynes has published in peer-reviewed journals on the topic (I’ll see what I can find) but this seems like another case of popular media grossly over-estimating (or mis-estimating?) the significance of the research. Take this excerpt:
But scientists are making enough progress to make ethicists nervous, since the research has already progressed from identifying the regions of the brain where certain thoughts occur to identifying the very content of those thoughts.
Although I think my favorite part is the opening paragraph, where the author writes:
At a laboratory in Germany, volunteers slide into a doughnut-shaped MRI machine and perform simple tasks, such as deciding whether to add or subtract two numbers, or choosing which of two buttons to press.
They have no inkling that scientists in the next room are trying to read their minds — using a brain scan to figure out their intention before it is turned into action.
Um…I think the first “inkling” that something is amiss is when these evil scientists ask you to step inside their big shiny machine. Perhaps I’m overly-critical. I still think articles like this are amusing, but it makes me cringe when I think that this is the public’s view of MR research. Any other opinions?
The following just came out over the SMRT mailing list:
Vendor issues new warning on Omniscan MR contrast for patients with kidney disease
GE Healthcare warned European providers Feb. 7 to discontinue the use of gadodiamide (Omniscan) for patients who may be at risk for a rare and life-threatening skin disease.
read the rest of the press release below the fold. (more…)
In December, an MRI machine exploded due to a liquid nitrogen leak:
Two workers moving an MRI machine were injured Thursday after an explosion blew part of the machine into a wall. The workers were moving the machine at Atlanta Diagnostic Center in Kennesaw, said Firefighter Denell Boyd, a spokeswoman for the Cobb County Fire and Emergency Services Department. Boyd said liquid nitrogen leaked from the machine and caused the blast, knocking a 10-foot by 10-foot hole in the wall.
Several photos of the damage to the facility were taken by the MRI techs and distributed on the SMRT mailing list. Copies of these photos below the fold: